
This website uses cookies so that we can offer you the best possible user experience. Some cookies are minimally necessary for the website to work. More information about cookies can be found here.

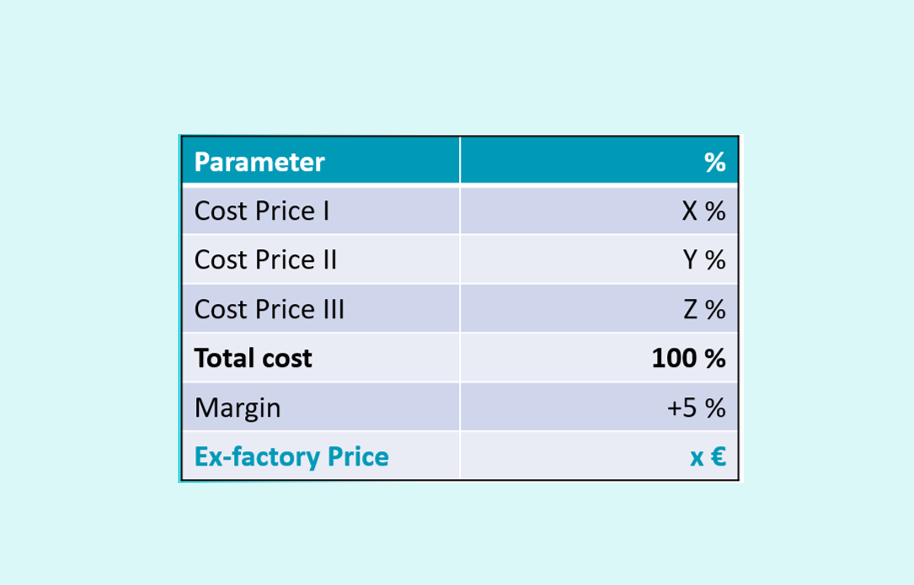
How to prove the concerned price if the specialty is not yet produced? What is the value of a proven pricing structure if the price is downsized over time? Lets discuss to overcome this bottleneck.
You dive into a simulation model and at first everything seems flawless. But with each adjustment the risk of flaws creeping into the programming.

The 'ICER' is a well-known measure to assess the extra cost to invest to win one QALY. In Belgium, unofficially 35 000 € / QALY gained is often applied as benchmark, the 'willingness to pay' (WTP). But does the payer invest the budget in function of the potential medical need or not ?
How to prove the ‘added value’ when the concerned innovation is beneficial without producing ‘health’ in a direct way?
How to indicate if an innovation is worthwhile to pay for in view of the claimed benefit it will bring? The goal of the NMB is to compare two interventions by subtracting the NMB of ‘intervention A’ from the NMB of ‘intervention B’, resulting in the incremental NMB (iNMB).
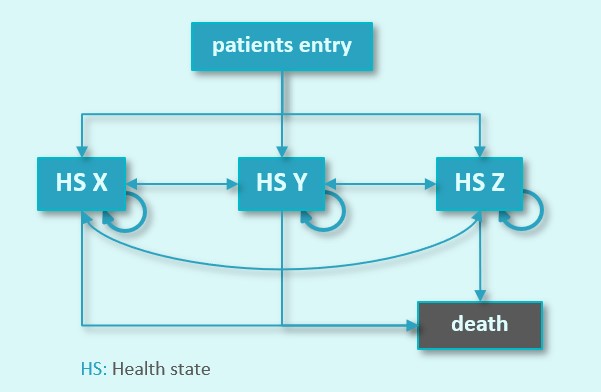
Always wondered how health economic models work? Good news: this blog is developed to guide you through the basic elements of ‘health state transition models’.

To estimate a launch date, some questions will pop-up. Based on the answers, (in combination with a strong strategy) a realistic estimate of the procedural time will become valid.

All market access colleagues involved in the preparation of economic files will be confronted with the aspect of inflation. There are 2 viewpoints versus ‘today’.

We all know that the pathway between the ‘eureka’ moment and the implementation is long. If needed the regulatory bodies can decide to initiate a ‘fast track procedure’.